ASW Report: Vague Legislation and Weak Data Mislead the Public on Physician-Assisted Suicide
America Is Not Getting the Full Story on PAS

Summary
Physician-assisted suicide (PAS) is often presented as a simple, peaceful, and humane way to avoid pain and suffering at the end of life. This paper contrasts the misleading language used by PAS advocates with the actual legislative verbiage to illustrate how the legal formation of PAS never matches the initial rhetoric. Second, it shows the failures of state statutory language by examining the annual state data reports from states where PAS is legal.
The paper demonstrates the following:
-
- PAS legislation is vague in its definitions and restrictions, and provides multiple loopholes that put vulnerable demographics at risk of abuse or coercion.
- The terminally ill safeguard fails to limit who can receive a prescription for PAS.
- The mental capacity safeguard fails to protect those who may be suffering from impaired judgment.
- Though “inadequate pain control” is one of the main arguments used to pass PAS legislation, not only is it not a primary reason people choose PAS, but the number is likely significantly inflated.
- PAS legislation effectively prevents oversight through the “good faith provision” and the requirement to put the patient’s underlying illness as the cause of death.
- Side effects of the lethal drug combinations used to kill patients are downplayed and lack any form of regulation, creating a serious safety risk.
- PAS legislation and data collection do not provide enough oversight to prevent abuse and coercion, causing both to go unnoticed with no consequences.
The legislative statutes and current method of data collection prevent American citizens from understanding the true harms of PAS. The statutes’ inability to close multiple loopholes shows an utter disregard for the wellbeing of America’s most vulnerable, and the lack of clarity in the data inhibits the ability to have an open conversation about PAS. Ultimately, this distracts from care-centered discussions on issues like advance care planning and hospice or palliative care.
Part I: The Impotence of Physician-Assisted Suicide Legislation
PAS is legal in 12 U.S. jurisdictions.[1] What was originally a controversial issue after being legalized in Oregon in 1997 has progressed rapidly in the past decade and continues to find its way into numerous state legislatures every year. And yet, this expansion comes in the midst of a major effort to prevent suicide in the United States, with the national 988 project responding to what the Surgeon General has deemed, “a national crisis.”[2] Why is suicide with a physician’s help suddenly seen as dignified, and even heroic? What changed?
Why do people want this?
Americans hold a place of high honor for individual achievement. Athletes, actors, and innovators reflect “The American Dream,” where if you work hard and overcome life’s obstacles, you can control your destiny and climb to the top of the social mountain, plant your flag, and make your mark on history. However, when this rugged individualism is deified, dependency becomes weakness, the vulnerable become burdens, and loneliness becomes the norm, plaguing certain cohorts of society more than others.
This attitude is acute among the Baby Boomers, a generation taught to prioritize the power of self-assertiveness and independence in post-World War II America.[3] But now they are forced to acknowledge the reality of aging and end-of-life care, and nothing challenges the mantra of individualism like aging and illness. So, when advocacy groups push PAS on them as a new, painless, and dignified solution for end-of-life care, offering one last chance to be in control, it seems too good to be true. Of course, it is neither.
PAS Legislation: A Utopian Vision
Advocates for PAS try to quell fears by claiming that so called “ethical guardrails” limit access to only those with a terminal illness, who can self-ingest, and are mentally capable, and promise a peaceful death while you sleep, free from abuse and coercion. At least, that’s the pitch. It’s one final stand for personal autonomy.
PAS Legislation: A Dystopian Mess
But PAS legislation reveals the practice is not so cut and dried as people assume. The language used in the legislation shows that the guardrails are weak, multiple loopholes exist, and patient well-being is an afterthought.
Begin with the definition of physician. An “attending physician” is “the physician who has primary responsibility for the care of the patient and treatment of the patient’s terminal disease.”[4] However, there is no indication that the patient needs to have an existing relationship with this physician, permitting “doctor shopping” where a patient can go to as many physicians as possible until they find one willing to prescribe them PAS.
“Doctor shopping” – Seeing multiple treatment providers, either during a single illness episode or to procure prescription medications illicitly.[5]
The same flaw applies for determining the patient’s prognosis. Legislation defines “terminal” as “an incurable and irreversible disease that has been medically confirmed and will, within reasonable medical judgment, produce death within six months.”[6] Can we rely on the accuracy of a prognosis from a medical professional who often has no previous relationship with the patient, when studies show that a majority of life expectancy prognoses are inaccurate?[7] These professionals are human, after all.
Moreover, what diseases are considered “incurable and irreversible?” Many people with disabilities have diseases that are both incurable and irreversible, but through modern medicine are able to live much longer than they otherwise would. Do these people automatically qualify if they decide that they are no longer going to take the medicines keeping them alive? Legislation provides no guidance. The influential bioethicist and PAS advocate Thaddeus Pope believes that by voluntarily stopping eating and drinking (VSED), one could qualify for assisted suicide. [8] Colorado physician Jennifer Gaudiani admitted in a report to prescribing PAS to patients who had anorexia as their sole condition. [9] It’s no surprise that every major national disability rights organization opposes PAS.[10] Add the fact that the legislation often does not require psychiatric referrals and it is easy to see why there is a major risk for coercion.[11]
Making matters worse, at the time of ingestion of the lethal medicine when a medical professional’s presence is most necessary, a physician is not required to be present. So, it can’t be confirmed that the “self-ingestion” safeguard was followed, nor can it be confirmed if a victim suffered traumatic complications from the experimental poisons involved.[12] The promise of death in a “humane and dignified manner” is only used to convince people of the “benefits” of PAS when in reality these drug combinations have not been studied and are not FDA approved.[13] Legislation also provides no way of ensuring that unused poisons are disposed of properly which otherwise is a huge health risk since the most common drug combination used in PAS, DDMAPh, contains sixty times the average lethal dose of morphine.[14]
The most disturbing aspect of this lack of oversight is the “good faith” provision which states that “no person shall be subject to civil or criminal liability or professional disciplinary action for participating in good faith compliance.”[15] This is the biggest loophole of all because as long as those involved in PAS claim that they were acting in good faith, regardless of abuse or medical malpractice, they aren’t subject to civil or criminal liability.[16] This “good faith” provision is present in seven state statutes.[17] Because victims inevitably die from ingestion of poison, such cases of abuse or coercion are impossible to confirm and punish. Why is this “good faith” provision necessary? If the goal is to die on your own terms and someone is robbed of this through someone else’s negligence, it should be more difficult for the perpetrator to get off clean. Is this law for the sake of the patients, or those who hasten their deaths?
“No person shall be subject to civil or criminal liability or professional disciplinary action for participating in good faith compliance.”
The nail in the coffin is that death certificates for those who commit PAS must list the underlying illness as the cause of death and not the actual cause of death – PAS. Why the deception and cover-up? Doesn’t the patient, by ingesting lethal drugs, get to choose when they die, and not the illness? Why not reflect that on death certificates? This is just another way to hide abuse or coercion, which can’t be tracked when it is unknown whether or not someone died from PAS.
This is dignity?
For a law that promises death on one’s own terms, the risks of coercion and abuse through all the loopholes available are clearly more prominent than advertised. With only a brief overview of the legislation, it’s hard to be convinced that this is really “death with dignity.” Before even looking at the impact of these laws, the very language of these laws invites suspicion. Touted safeguards are simply gates with broken locks, not impenetrable walls, coercion and abuse are impossible to track, and a “peaceful death” is not guaranteed.
Shouldn’t the administration of lethal drugs require greater due diligence and oversight when life and death are literally on the line? Everyone should have the right to age and die with dignity, but having healthcare professionals poison patients to avoid burdening others is not how that is achieved. That’s why the American Medical Association, America’s most prominent association of physicians, just reaffirmed their long-held stance that “physician-assisted suicide is fundamentally incompatible with the physician’s role as healer.”[18]
“Physician-assisted suicide is fundamentally incompatible with the physician’s role as healer, would be difficult or impossible to control, and would pose serious societal risks.” – AMA
Part II: The Wild West of PAS Data
It is clear that loopholes exist, but do they actually matter? In every state where PAS is legal, the law requires that a statistical report be regularly released to monitor usage and ensure compliance with state law.[19] These reports are intended to convince the reader, whether it be a member of congress, a physician, or simply the average American that PAS is safe and can be implemented on a national scale. However, a convincing argument must be based on reliable data, and America’s PAS data is a mess.
Every state hails Oregon’s initial law as the model for PAS legislation, but not a single state follows its reporting method (which is itself inadequate). State reports range anywhere from two to nineteen pages; California bases its data on the number of people who died through the ingestion of lethal drugs while Washington, who in an apparent violation of its state statute just announced it will stop reporting altogether, based it on how many applicants died regardless of ingestion status; Vermont releases its data every other year; New Mexico has never released a report in the four years since it legalized PAS; Oregon tracks over twenty different demographic categories while Maine lists fewer than ten. And while some reports are specific in describing underlying illnesses or the kinds of lethal drugs used, others stick to general terminology, which makes collecting cumulative data impossible.
Yet, despite this lack of congruity in the state data reports, the data makes clear that PAS is not the harmless practice romanticized by Hollywood and the media.
What do the numbers say?
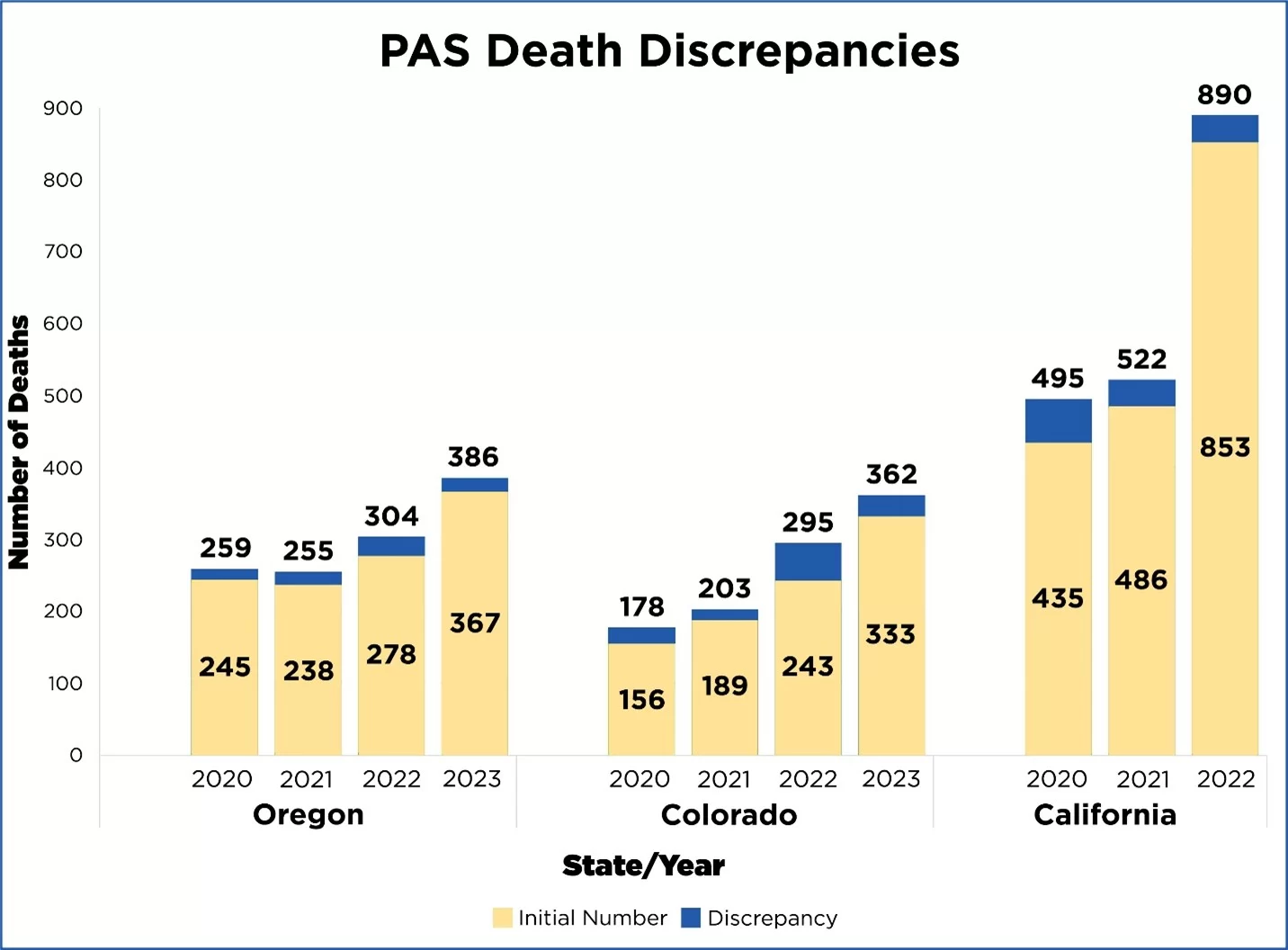
Advocates call PAS a “trusted and time-tested medical practice that allows a terminally ill, mentally capable adult with a prognosis of six months or less to live to request from their doctor a prescription for medication they can decide to self-ingest to die peacefully in their sleep.”[20] How trustworthy a practice is it? Year-over-year data reveals death toll discrepancies as high as 21%.
As far as being only for the terminally ill, Americans might be shocked to discover that many people with non-terminal conditions used PAS to end their lives. Data from Oregon, California, and Colorado reveal that ailments such as arthritis, a hernia, diabetes, and even “complications from a fall” qualified individuals for PAS.[21] A 2024 report from Eat Breathe Thrive, a non-profit helping people recover from eating disorders, unveiled multiple cases in the United States (and over 60 internationally) of people who solely on the basis of their anorexia died by assisted suicide.[22] But, for some reason this information is hidden in the data reports under the catch-all category of “other,” consigned to footnotes, or simply omitted.
And the reported protection of the “mentally capable” safeguard present in every state’s statute also has failed. Oregon, the only state that collects and publicly reveals psychiatric referral percentage data, shows that less than 1% of people in 2024 received a psychiatric referral.[23] This means that over 99% of patients who received suicide-affirming care were believed to have no mental health issues, when studies show that receiving a terminal diagnosis can cause depression in up to 77% of people.[24]
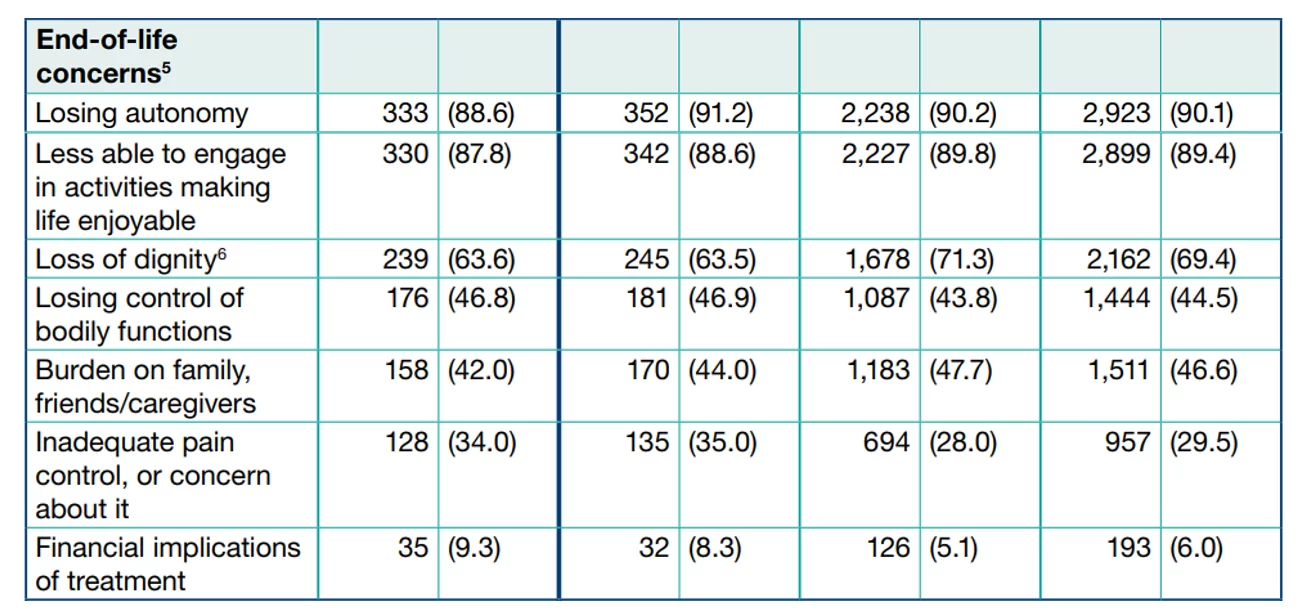
Advocates argue that PAS is still necessary because no one should have to experience unbearable suffering at the end of life. Though only a few states track the actual reasons why people choose to pursue PAS, the data shows that inadequate pain control is not one of the top reasons. The desire for autonomy, and the fear of being a burden are the principle motivations. In Oregon inadequate pain control is listed as a reason in less than 35% of the cases, and even this number is deceptive because the category addresses not only inadequate pain control but also “concern about it.” More alarming is the fact that “financial implications of treatment” has increased a full seven percentage points in the past ten years, from 2.3% to 9.3%, while concern for pain has increased five, further revealing that the problem extends beyond more than just the fear of pain.[25]
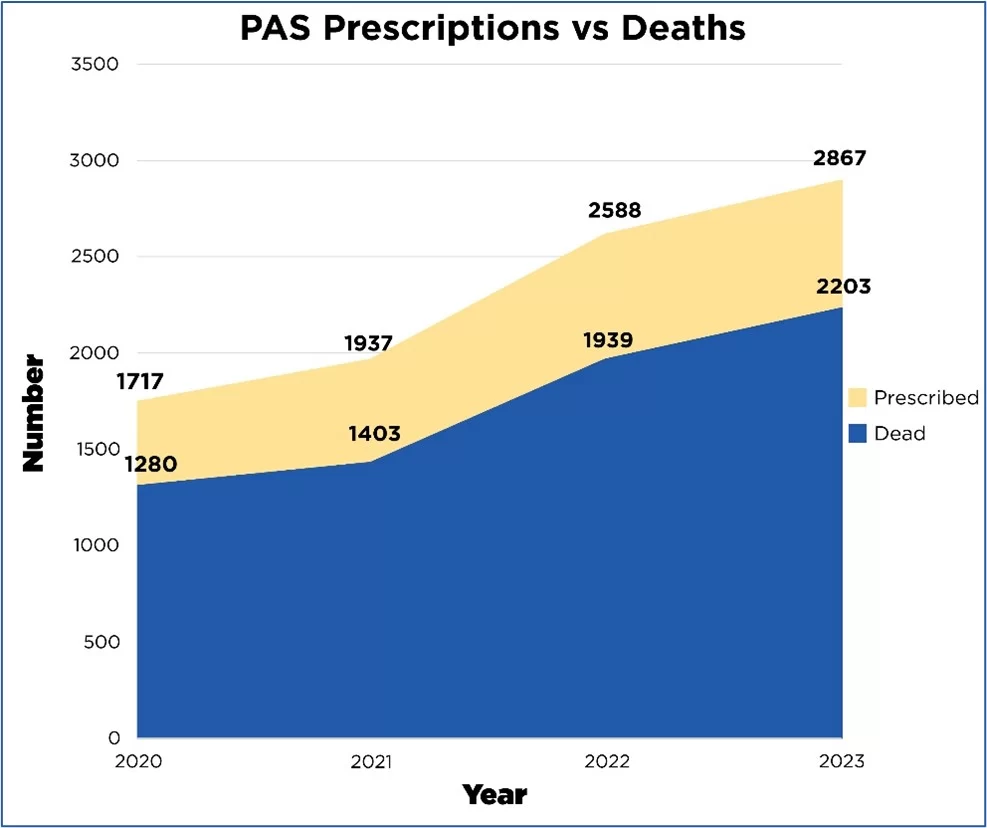
PAS also fits into the distinctly American flaw of our healthcare system which tends to overmedicate. Though there is no agreed-upon drug combination, the drug cocktails used cause intense burning sensations in the throat, vomiting, and seizures.[26] Plus the complication rate of these cocktails is very high. Data on the complication rate is available for less than half of PAS deaths but the known complication rate for PAS is 7% and was almost 10% in 2024.[27] Moreover, data from Oregon and California alone reveal that thousands of prescribed lethal drugs have gone unaccounted for, presumably just lying around in patient’s homes, leaving patients, their friends, and their families at serious risk, especially in the midst of a national pain-killer abuse crisis according to the U.S. Department of Health and Human Services.[28]
Among all the statutory frameworks that legalize PAS, not a single state has a mechanism to improve the lax regulations surrounding this deadly practice, and data collection does not provide remotely enough oversight. Even if data collection is improved, the flawed legislation remains, leaving the door open for abuse and coercion. In an email to Assisted Suicide Watch, a representative from Colorado’s Department of Public Health and Environment admitted as much about its oversight capabilities stating, “While reporting is required through Colorado Board of Health rule, there’s little teeth behind it.”[29] Oregon’s overview of its reporting method states, “Because physicians are not legally required to be present when a patient ingests the medication, not all have information about what happened when the patient ingested the medication.”[30] Not a single state provides an annual report on instances of abuse, despite the high rate of elderly abuse in America, the age demographic using PAS the most.[31] Coercion and abuse simply go unnoticed.
Conclusion
PAS has been in the United States since the late 20th century, but remains poorly understood by most Americans. The legislation and resulting data reports are intentionally vague because if they were in-depth, they would reveal that PAS is false compassion wrapped in the guise of “dignity” and “autonomy.” Though advocates for PAS present it as safe and peaceful, this characterization is contradicted by the data, which reveals a seriously flawed practice nowhere near as clear-cut as we are told. The reports alone are proof that PAS legislation has no intention of protecting the vulnerable. The only thing it accomplishes is turning physicians against their oath to “do no harm.”[32]
Death is so much more than just a medical moment and PAS is the wrong answer to the false choice of a peaceful suicide or endless agony. People can have their emotional, personal, and spiritual needs met through better and more accessible palliative care that promotes life instead of ending it. The message conveyed by PAS advocates is that dignity at the end of life can only be achieved once PAS is legalized, but weak legislative language, lack of oversight, and murky data reports make it clear that when PAS is put into practice, the mess is the real message.
[1] CA, CO, DC, DE, HI, ME, MT, NJ, NM, OR, VT, WA
[2] Department of Health and Human Services. “The surgeon general’s call to action.” https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
[3] Johns Hopkins University. “The changing generational values.” (2022, November 17). https://imagine.jhu.edu/blog/2022/11/17/the-changing-generational-values/.
[4] Oregon Health Authority. “Oregon revised statute: Oregon’s death with dignity act.” (2023). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Pages/ors.aspx.
[5] Randy, S., & Lori, S. “Doctor shopping: A phenomenon of many themes. Innovations in clinical neuroscience.” (2012, November 9). https://pubmed.ncbi.nlm.nih.gov/23346518/.
[6] Oregon Health Authority. “Oregon revised statute: Oregon’s death with dignity act.” (2023). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Pages/ors.aspx.
[7] Higginson, Irene J., & Costantini, Massimo. “Accuracy of prognosis estimates by four palliative care teams: A prospective cohort study.” (2002, March 4). https://pmc.ncbi.nlm.nih.gov/articles/PMC88964/.
[8] Briscoe, Joshua & Widera, Eric. “Law not loopholes: Medical aid in dying for those with dementia.” (2024, February 26). https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.18828.
[9] Gaudiani, J. L., Bogetz, A., & Yager, J. “Terminal anorexia nervosa: Three cases and proposed clinical characteristics – journal of eating disorders.” (2022, February 15). https://jeatdisord.biomedcentral.com/articles/10.1186/s40337-022-00548-3.
[10] Not Dead Yet. “Disability groups opposed to Assisted Suicide Laws.” https://notdeadyet.org/disability-groups-opposed-to-assisted-suicide-laws/.
[11] Oregon Health Authority. “Oregon revised statute: Oregon’s death with dignity act.” (2023). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Pages/ors.aspx.
[12] Disability Rights Education and Defense Fund (DREDF). “Some Oregon and Washington State Assisted Suicide Abuses and Complications.” https://dredf.org/wp-content/uploads/2015/04/Revised-OR-WA-Abuses.pdf.
[13] Oregon Health Authority. “Oregon revised statute: Oregon’s death with dignity act.” (2023). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Pages/ors.aspx. (“Humane and dignified manner” is mentioned 18 times)
[14] Li, Juntao, et al. “Forensic aspects about fatal morphine intoxication of an unusual body packer: Case report and literature review.” (2021, May 12). https://www.sciencedirect.com/science/article/pii/S2665910721000384.
[15] Oregon Health Authority. “Oregon revised statute: Oregon’s death with dignity act.” (2023). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Pages/ors.aspx.
[16] Hendin, Herbert & Foley, Kathleen. “Physician-Assisted Suicide in Oregon: A Medical Perspective.” (2008). https://repository.law.umich.edu/cgi/viewcontent.cgi?article=4363&context=mlr.
[17] CA, CO, DC, NJ, NM, OR, WA
[18] AMA Code of Medical Ethics. Physician-Assisted Suicide. https://code-medical-ethics.ama-assn.org/ethics-opinions/physician-assisted-suicide
[19] Compassion & Choices. “Medical aid-in-dying utilization report.” https://compassionandchoices.org/resource/medical-aid-in-dying-utilization-report/
[20] Compassion & Choices. Medical aid in dying. https://compassionandchoices.org/our-issues/medical-aid-in-dying/
[21] Oregon Health Authority. “2020 Oregon Death with Dignity Act Data Summary.” (2021, February 26). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Documents/year23.pdf.
[22] Roff, C. & Cook-Cottone, C. “Assisted death in eating disorders: A systematic review of cases and clinical rationales.” (2024, July 30). http://frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2024.1431771/full.
[23] Oregon Health Authority. “2024 Oregon Death with Dignity Act Data Summary.” (2025, March 27). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Documents/year27.pdf.
[24] Cirino, Erica. “Depression in the face of a terminal illness and death.” (2018, February 28). https://www.healthline.com/health/depression/terminal-illness.
[25] Oregon Health Authority. “2024 Oregon Death with Dignity Act Data Summary.” (2025, March 27). https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Documents/year27.pdf.
[26] Worthington, A., et al. “Efficacy and safety of drugs used for ‘assisted dying.’” (2022, May 4). https://pmc.ncbi.nlm.nih.gov/articles/PMC9270985/.
[27] Calculations based on Oregon data.
[28] U.S. Department of Health and Human Services. National opioids crisis: Help and resources. https://www.hhs.gov/opioids/index.html
[29] Mentioned in an email exchange between Colorado’s Department of Health and Environmental Data and Aging with Dignity. (November 18, 2024).
[30] Oregon Health Authority. “Oregon Methods.” https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Documents/methods.pdf
[31] World Health Organization. “Abuse of older people.” (2024, June 15). https://www.who.int/news-room/fact-sheets/detail/abuse-of-older-people.
[32] OMNIKA Foundation Contributors. “”The Oath”: English Translation of Hippocratic Oath by William H. S. Jones.” OMNIKA – World Mythology Index, OMNIKA Foundation, (2019, May 15). https://omnika.org/texts/158.